 Whatever treatment you decide to pursue for spinal related pain, it is important that the doctor you see takes a thorough history of your pain and symptoms, does functional exams to clinically correlate your pain and then orders imaging to confirm or rule out the suspected cause of your pain. The order should be:
Whatever treatment you decide to pursue for spinal related pain, it is important that the doctor you see takes a thorough history of your pain and symptoms, does functional exams to clinically correlate your pain and then orders imaging to confirm or rule out the suspected cause of your pain. The order should be:
- HISTORY/COMPLAINTS
- FUNCTIONAL/STRUCTURAL EXAM
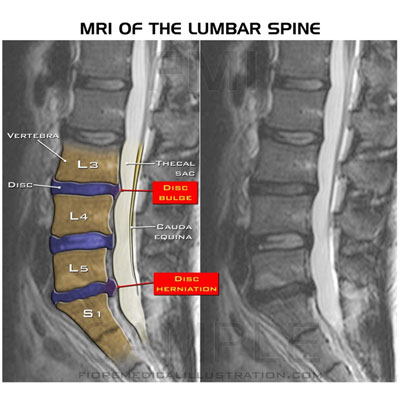
- IMAGING based on what is suspected to be the problem.
This ABC approach is what leads to an accurate diagnosis.
Treatment options should be considered only after an accurate diagnosis is obtained and not based on just A or B or a guess. Causes of spinal pain can vary: disc, nerve root compression, spinal cord compression, facet/joint pain, altered biomechanics and muscular just to name a few.
Treatment options vary depending on the diagnosis but most spinal pain options follow this general order from
CONSERVATIVE CARE
Medication – anti-inflammatories, muscle relaxers, opioids (pain killers), anticonvulsants (Neurontin)
Physical therapy – strength and flexibility of the supporting spinal muscles
Chiropractic – spinal biomechanical issues (mechanical spine pain)
Rest – backing off activity that aggravates the condition, using ice for inflammation and heat for muscle spasm
MODERATE CARE
Epidural Steroid Injection – injecting a steroid to reduce nerve root irritation (bathes nerve root in steroids). Needle is guided by fluoroscopy to ensure accuracy. Typically done with an interlaminar approach (more medial) or transforaminal (more lateral) near nerve root itself
Facet Block Injection – injection into the joint (intraarticular) or blocking the nerves near a joint (medial branch block)
Rhizotomy – needle is used to cauterize (burn) pain sensors (nociceptors) on the facet surface of a spinal joint that transmit pain
Spinal Cord Stimulator – implantable device that modulates pain by sending electrical signals to select areas of the spinal cord
Morphine pump – infuses morphine into the spinal fluid when maximum conservative and surgical treatment has failed
SURGERY
Minimally invasive surgery – make small incisions and operate through a small tube or endoscope to remove debris and decompress the pressure on the nerve and/or remove disc material and other anatomy causing compression. Does less damage to normal tissue than traditional surgery and usually involves a smaller incision and quicker recovery time. Preferred method if clinically indicated.
Traditional Back Surgery – laminectomy (removing posterior portion of spinal column to remove pressure), discectomy (removing portions of the disc that are compressing the nerve), and possible fusion to stabilize the spinal region. Typically requires cutting through normal tissue and has longer recovery times because normal tissue is disrupted to get to the area that needs repair.